

Abstract
Background: Assessment of the musical ability of people with schizophrenia has attracted little interest despite the diverse and substantive findings of impairments in sound perception and processing and the therapeutic effect of music in people with the illness. The present study investigated the musical ability of people with schizophrenia and the association with psychiatric symptoms and cognition.
Methods: We recruited patients with chronic schizophrenia and healthy controls for participation in our study. To measure musical ability and cognitive function, we used the Montreal Battery of Evaluation of Amusia (MBEA) and the Brief Assessment of Cognition in Schizophrenia (BACS). We carried out a mediation analysis to investigate a possible pathway to a deficit in musical ability.
Results: We enrolled 50 patients and 58 controls in the study. The MBEA global score in patients with schizophrenia was significantly lower than that in controls (p < 0.001), and was strongly associated with both the composite cognitive function score (r = 0.645, p < 0.001) and the negative symptom score (r = −0.504, p < 0.001). Further analyses revealed direct and indirect effects of negative symptoms on musical ability. The indirect effects were mediated through cognitive impairment.
Limitations: The relatively small sample size did not permit full evaluation of the possible effects of age, sex, education, medication and cultural influences on the results.
Conclusion: Examining the associations between musical deficits, negative symptoms and cognitive imapirment in patients with schizophrenia may identify shared biological mechanisms.
Introduction
Like language, music is a universal, human-specific cultural experience. Perception, interpretation and production of music are linked to language, emotion, cognitive function and social communication in everyday life. Neurocognitive and clinical studies have investigated musical emotion, cognition and musical disorders.1,2 Deficits in musical processing, or amusia, have been intensely investigated for more than a decade.3 Amusia can be identified by the Montreal Battery of Evaluation of Amusia (MBEA), used as a standard battery of tests for music assessment in people with acquired (secondary to brain injury or illness) or congenital (“tone deafness,” detectable early in childhood) forms of the disorder.4,5
Music perception and processing in healthy individuals are influenced by several factors, including sex, age, musical experience and cultural background. Sex differences have been observed in both children and adults when measuring early right anterior electrophysiological activity in processing musical information.6 Maturation of the brain through childhood, adolescence and early adulthood, and aging of the brain in elderly people have a wide range of effects on musical ability and on activation of specific brain regions while testing musical ability.7–9 Active musical training has distinct effects from those of maturation or aging.9 Culture and language effects can influence some parts of the MBEA, such as the metre test, and are also reported to alter the sensitivity of pitch perception.10,11
The association between musical ability and cognitive function has been investigated in patients with neurologic illnesses. In those with Alzheimer disease, musical performance is preserved to a greater degree than other mental activities and is relatively preserved even in the most severe stages of illness.12–14 Recent findings indicate middle cerebral artery stroke can cause acquired amusia,15–17 which is associated with auditory cortex and frontal lobe damage, with the expected patterns of cognitive impairment following damage to these regions.15 Three months after a stroke, improvement in musical deficit is linked to recovery of verbal learning, visuospatial perception and attention, suggesting that musical ability in people with acquired amusia is associated with multiple cognitive functions.15,16 In contrast to the large body of literature on the association of neurologic disorders and cognitive impairment with musical ability,18 less is known about the effects of severe mental illnesses.
Schizophrenia is a major mental disorder that manifests several core features, including positive symptoms, such as hallucinations and delusions, and negative symptoms, such as apathy and poverty of speech.19 In addition to clinically obvious psychiatric symptoms, schizophrenia is frequently complicated by neuropsychological or cognitive impairment, which can be as severe as clinical dementia.20 While the positive symptoms of schizophrenia show little association with cognitive impairment, the negative symptoms demonstrate a complex association with cognition in the illness.21,22 In most studies, negative symptoms and cognitive impairment covary, but these domains of illness appear to contribute to a distinct and interrelated pathway in predicting real-world functional impairment.21,23 However, negative symptoms are also present in the rare cases of schizophrenia where cognition is preserved at a superior level.24 Both symptoms and cognitive impairment in patients with schizophrenia may be related to abnormal sensory processing mechanisms, several of which are relevant to music and the brain.25 These include auditory event-related evoked potentials, such as P50, P300 and mismatch negativity.26–28 Dysfunction of auditory information processing and altered perception of pitch and intensity are also observed.29 Abnormalities in detection of the prosodic qualities of speech in patients with schizophrenia are linked to auditory pathways.30 The negative symptoms of schizophrenia are also associated with abnormalities in detecting frequency modulated tones designed to mimic key acoustic features of human vocal expressions.31
Exploration of the musical abilities of patients with schizophrenia may provide a unique opportunity to link the symptoms of illness to an important aspect of brain function. In this study, we used the MBEA, which is widely used for assessment of musical ability, to determine whether patients with schizophrenia have a deficit in musical ability. We examined associations between musical ability and sex, age, musical training, education and the characteristic symptomatology of schizophrenia. Finally, we carried out an exploratory mediation analysis to investigate the pathway from the symptoms of schizophrenia to musical disability. We were specifically interested in the possible role of a causal pathway from negative symptoms, mediated through cognitive impairments described in patients with schizophrenia, to music disability.32
Methods
Participants
We recruited patients with schizophrenia from 3 mental hospitals in the southwest of Japan. The patients had either schizophrenia or schizoaffective disorder, which was diagnosed according to ICD-10. Exclusion criteria were history of neurologic disorder and current substance abuse or dependence. We also recruited healthy controls from the community via advertisement. We obtained written informed consent from all participants after the study was described to them. The study was approved by the Ethics Committee of Kochi Medical School.
Measurement of musical ability
We used the MBEA to measure the musical ability of patients with schizophrenia and healthy controls. The MBEA is composed of 6 tests or subscales: Scale, Contour, Interval, Rhythm, Meter and Memory. Scale, Contour and Interval measure melodic ability, while Rhythm and Meter measure temporal ability. Each test uses musical phases designed to test specific abilities. The mean duration of each musical phrase is 5.1 (range 3.8–6.4) seconds, with the exception of the metric test in which phrases are twice as long. The phrases are presented with a piano sound. For examples and additional detail, see the Peretz laboratory website (www.brams.umontreal.ca). For the subscales of Scale, Contour, Interval and Rhythm, we presented 2 musical phrases in succession to the participant, who was then asked if the phrases were the same or different. For the Meter subscale, the participant was asked if the phrase was a march or a waltz. For the Memory subscale, the participant was asked if a presented phrase had already been presented. We presented participants with 30 questions for each subscale. All 6 sub-scale sessions were completed in approximately 1 hour, and we used the mean for the 6 scale scores as the global score. Chance level was 50% for all tests. The interviewer (S.H.) encouraged participants to respond to the tests, and good cooperation was obtained from all participants.
Assessment of mental state and cognitive function
To evaluate the symptoms of schizophrenia, patients were assessed using the Positive and Negative Syndrome Scale (PANSS), the Clinical Global Impression scales and the Global Assessment of Functioning (GAF) scale.33,34 To assess possible extrapyramidal motor side effects of antipsychotic medications, we used the overall severity score of the Drug-Induced Extrapyramidal Symptoms Scale (DIEPSS), including assessment of dyskinesia, akathisia, dystonia and Parkinsonism. Overall severity on the DIEPSS ranges from zero (normal) to 4 (severe).35 To examine cognitive functions, we used the Brief Assessment of Cognition in Schizophrenia; Japanese version (BACS).32
Statistical analysis
We evaluated data for normality using the Shapiro–Wilks test. Possible differences in demographic variables between patients and controls were assessed with Student t test for normally distributed variables or the Mann–Whitney U non-parametric test, as appropriate. We used similar approaches to test for differences in musical ability between patients and controls and between patients with normal musical ability and those with amusia. We set the amusia cut-off score as lower than 2 standard deviations (SDs) below the control mean MBEA global score (equating to 76.8% correct), which is very similar to the cut-off for amusia of 77.6% reported in the original description of the MBEA.5 We used partial correlations to examine the association between global musical score and clinical variables and cognitive functions, controlling for age and sex. For musical training, we used the Kendall τ statistic, and we used Pearson correlation coefficients for all other correlations. All analyses were performed using SPSS version 11 (SPSS Japan).
We conducted mediation analyses using the SPSS macro Indirect, as described by Preacher and Hayes.36 A mediation analysis is a test of a causal model, describing the extent to which an independent variable affects an outcome variable, through an intervening variable (a mediator).36,37 A logical ordering of the independent variable, mediator and outcome variable can often be specified based on their temporal ordering. In the present cross-sectional study of schizophrenia, establishing temporal ordering for the putative independent (symptoms) and mediator (cognition) variables was not possible. Because cognition is proximal to musical ability in various clinical conditions, we evaluated cognition as the mediator to account for the link between symptoms and musical abilities. The proposed mediation model is considered to be the most parsimonious (see the Introduction), but is not the only model that could be evaluated.38
Using bootstrapped standard errors, mediation is established if the 95% bias-corrected and accelerated confidence interval for the indirect effect does not include zero. We first examined total symptom severity to assess associations between total symptoms, cognitive function and musical ability. We then investigated the specificity of these findings to positive or negative symptoms. To estimate the effects of positive versus negative symptoms within the context of the potential intervening role of cognition (indirect effects), we conducted 2 multiple independent mediation analyses. In the first, positive symptom severity served as the independent variable, with the negative symptom score and age as covariates. For the second analysis, negative symptom severity was the independent variable, with the positive symptom score and age as covariates. In both analyses the direct effects of the symptom scores and the indirect effects of the cognitive mediator were established. Mediation analyses were controlled for possible effects of age.
Results
Participants
All participants were ethnic Japanese from Kochi Prefecture in the southwest of Japan. We enrolled 50 patients with schizophrenia and 58 controls in the study. All patients were treated with antipsychotics. The demographic and clinical characteristics of participants are summarized in Table 1. There was no significant difference in age or years of musical training (typically during childhood, ages 4–10 yr, most commonly a keyboard instrument, such as a piano) between the groups, but patients with schizophrenia had significantly fewer years of general education than controls. Twenty-two of 58 controls and 14 of 50 patients with schizophrenia had amateur musical training. As expected, the patient group showed significant cognitive impairment compared with the healthy control group (Fig. 1).
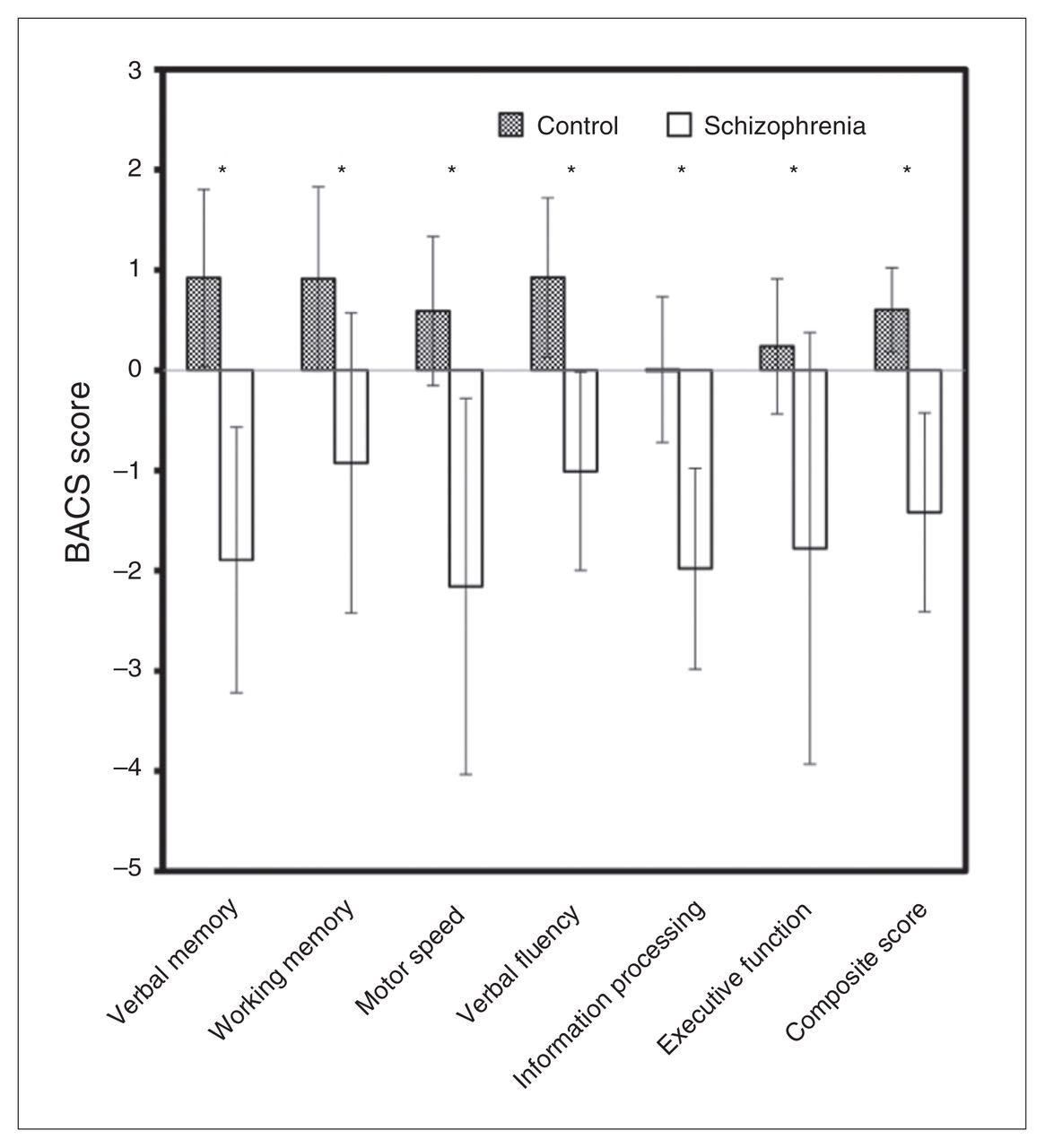
Brief Assessment of Cognition in Schizophrenia (BACS) composite and subscale scores. *p < 0.01, Student t test.
Demographics and clinical characteristics of patients with schizophrenia and healthy controls
MBEA scores
The MBEA global mean score differed between the groups (71.1% for patients with schizophrenia v. 88.4% for controls, t65 = 8.57, p < 0.001; Fig. 2A), and showed a normal distribution in each group, as reported elsewhere.5 In addition, for all 6 MBEA subscales shown in Fig. 2A, the patient group had lower scores than the control group (all p < 0.001). Rhythm, Meter and Memory scores were not normally distributed in the control group (likely owing to ceiling effects); all scores in the musical subcategories were normally distributed in the schizophrenia group. Three of 58 (5.2%) controls and 31 of 50 (62%) patients with schizophrenia satisfied the amusia criteria. Patients with and without amusia, respectively, differed in age (mean 41.8 ± 8.6 yr v. 54.3 ± 8.6 yr, t48 = 4.95, p < 0.001), years of education (mean 11.5 ± 1.9 yr v. 13.2 ± 2.4 yr, t48 = −2.79, p = 0.008) and duration of illness (mean 26.6 ± 9.1 yr v. 18.6 ± 11.4 yr, t48 = 2.75, p = 0.008).
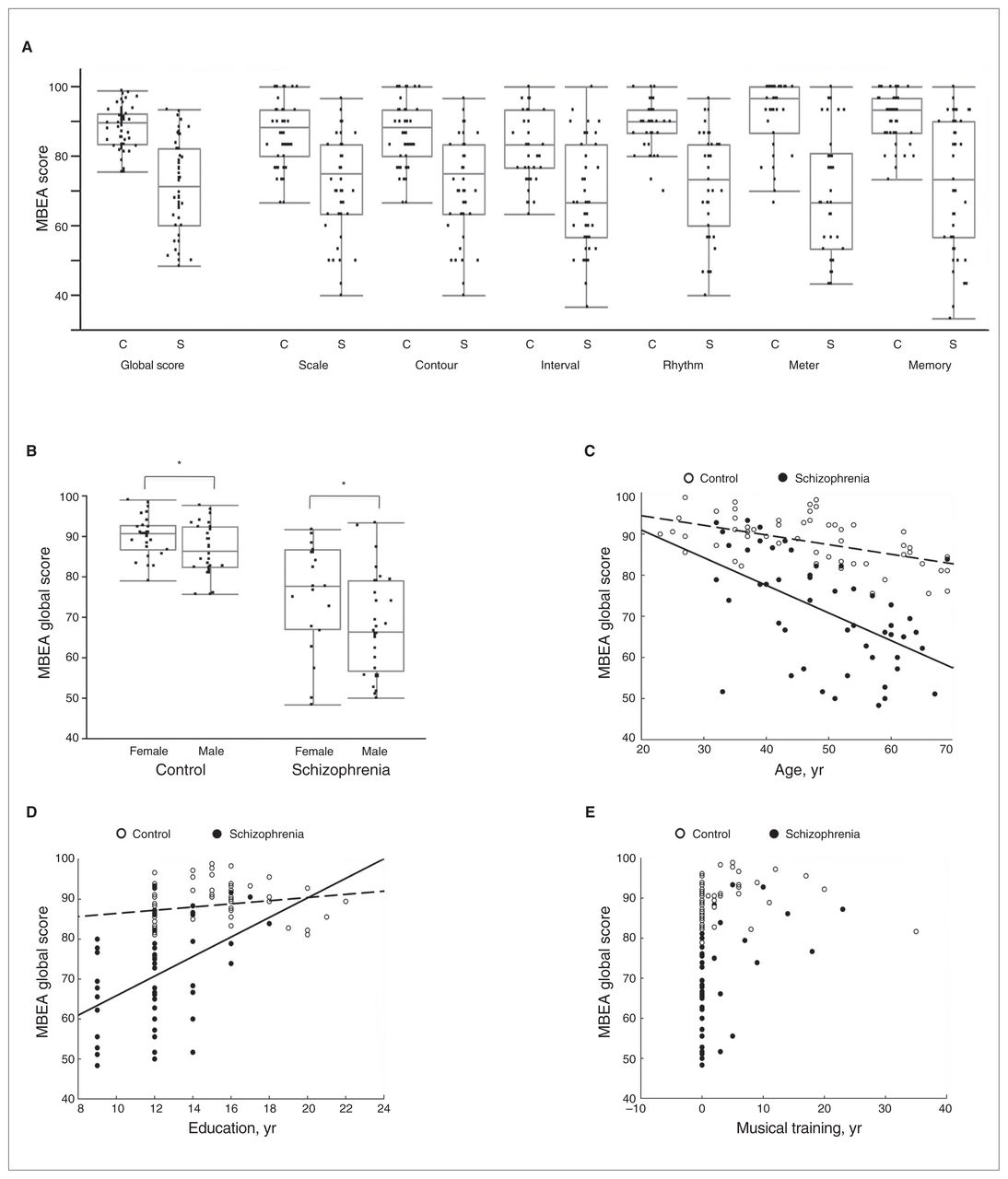
(A) Montreal Battery of Evaluation of Amusia (MBEA) global score and its subscales, (B) MBEA global score and sex, and MBEA global score with (C) age, (D) years of education and (E) years of musical training. Dashed regression lines in panels C and D refer to controls, and solid lines refer to patients with schizophrenia. C = controls; S = patients with schizophrenia. *p < 0.05.
Correlations with MBEA global score
To identify possible variables linked to musical disability, we analyzed the effect of sex on musical ability and the correlation of the MBEA global score with age, education and musical training, as shown in Figure 2B–E and Table 2. The MBEA global score for women was higher than that for men in both the control group (90.0% v. 86.8%, t56 = 2.18, p = 0.033) and the schizophrenia group (75.8% v. 68.0%, t48 = 2.14, p = 0.038; Fig. 2B). The global MBEA score was significantly associated with age in both controls and patients with schizophrenia (Table 2 and Fig. 2C), with years of education only in patients with schizophrenia (Table 2 and Fig. 2D), and with years of musical training in both controls and patients with schizophrenia (Table 2 and Fig. 2E).
Association of Montreal Battery of Evaluation of Amusia global score with demographic and clinical characteristics
Association of clinical features of illness and severity of symptoms with MBEA global score
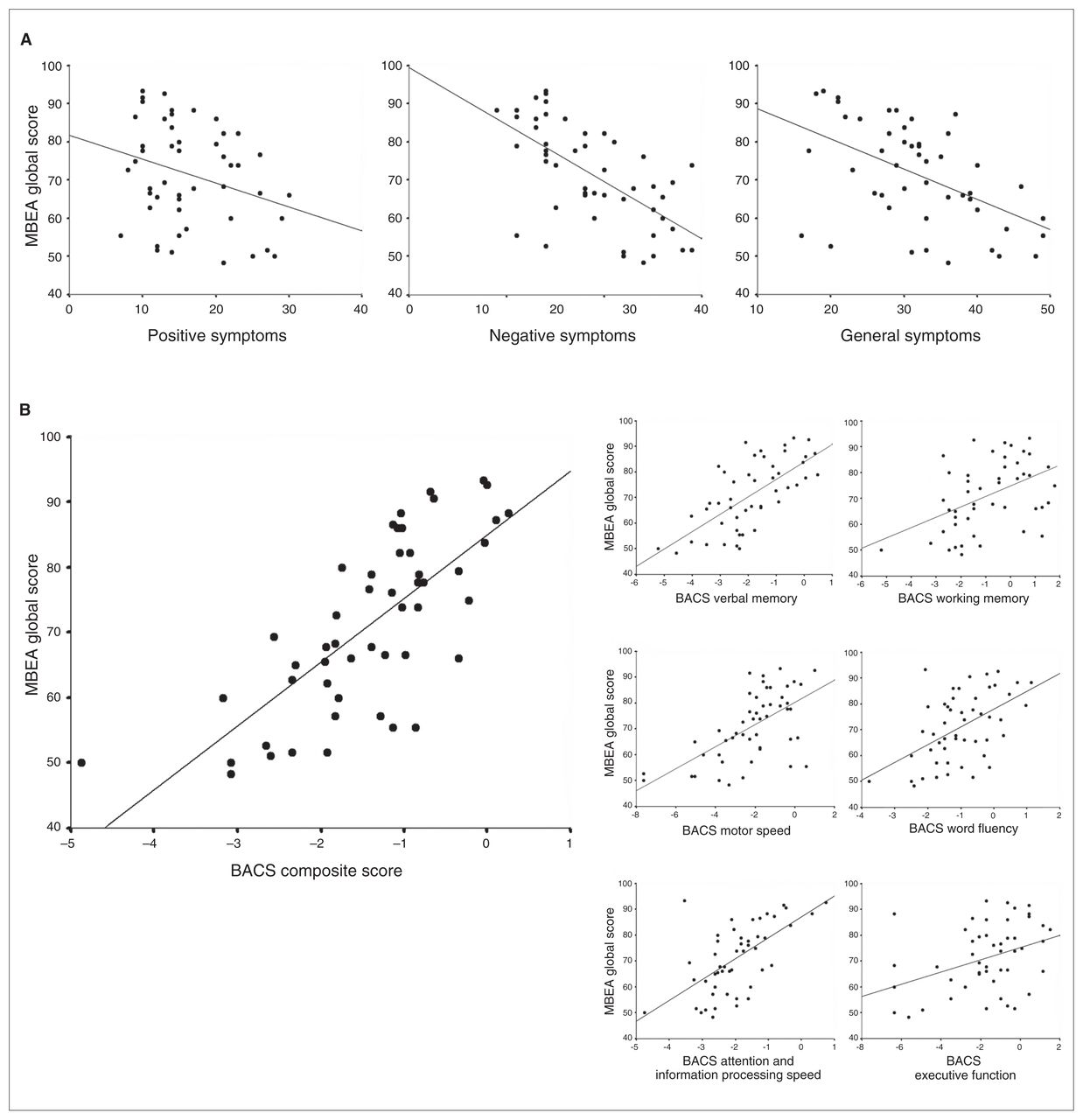
We first examined the effect of clinical features of illness and severity of symptoms on MBEA global score using partial correlation analyses. These were followed by analyses related to cognitive function. In the mediation analysis, we considered both symptom severity and cognitive function. Lower negative and general psychopathology symptom scores on the PANSS and higher scores on the GAF (both indicating milder psychopathology) were associated with higher MBEA global scores (Table 2 and Fig. 3A). Other correlations between clinical variables and the MBEA global score were not significant. Of note, antipsychotic medications are more effective in treating positive rather than negative symptoms of schizophrenia, which is consistent with the lack of association between medication dose and MBEA global score.

(A) Montreal Battery of Evaluation of Amusia (MBEA) global score and Positive and Negative Syndrome Scale subscale scores in schizophrenia, and (B) MBEA global score and the Brief Assessment of Cognition in Schizophrenia (BACS) composite and subscale scores in patients with schizophrenia.
Association of musical ability with cognitive function
Statistical analysis and scatter plots demonstrating associations between cognitive impairment and MBEA global score in the patient group are shown in Table 2 and Figure 3B. A partial correlation study of the schizophrenia group showed a significant association between MBEA global score and the composite score of the BACS. In the subtests of patients with schizophrenia, there were significant associations between musical score and all cognitive functions. As seen in the Appendix, Table S1, available at cma.ca/jpn, symptom severity was also associated with cognitive impairment.
Direct and indirect effects of psychopathology on musical ability in patients with schizophrenia
To evaluate the associations between global symptom severity, specific symptom types, cognitive function and musical deficits, we performed mediation analyses using 3 models (Appendix, Figure S1, and Table 3). Model 1 employed the PANSS total score as the independent variable, the MBEA global score as the outcome and the composite BACS score as the mediation variable, whereas models 2 and 3 used the PANSS positive and negative symptoms scores as multiple independent variables.
Bootstrap results for indirect effects of symptom severity on the Montreal Battery of Evaluation of Amusia global score via the Brief Assessment of Cognition in Schizophrenia composite score in 50 patients with schizophrenia, controlled for age and sex
In model 1 (Appendix, Fig. S1, and Table 3), mediation analysis based on 10 000 bootstrapped samples showed that after controlling for age and sex, the PANSS total score had an indirect effect operating through the BACS composite score (ab paths). The indirect effect accounted for approximately 48% (−0.145 of −0.302) of the total effect.
Next, in models 2 and 3, we assessed the extent to which cognitive function mediated the effects that positive and negative symptoms have on musical ability. In model 2, the PANSS positive symptom score had no significant direct or indirect effect on musical ability after controlling for the negative symptom score, age and sex. In contrast, in model 3, the PANSS negative symptoms score had both a significant direct effect on musical ability and an indirect effect on musical ability that was mediated by the BACS composite score after controlling for the effect of positive symptoms, age and sex. The indirect effect accounted for about 43% (−0.445 ÷ −1.030) of the total effect.
Discussion
The MBEA global score was lower in patients with schizophrenia than in controls. Clinical features of schizophrenia associated with poorer musical ability were higher severity of symptoms and lower global functioning. In patients with schizophrenia, greater cognitive impairment was associated with poorer musical ability. Mediation analyses showed that negative symptoms in patients with schizophrenia have both direct and indirect effects on musical disability, with the indirect effect mediated through cognitive impairment.
We found a markedly lower mean MBEA global score in the schizophrenia group than in the control group, and 62% of patients with schizophrenia were categorized as having amusia compared with 5% of control participants. The latter finding is consistent with a reported 3%–4% estimate of amusia in Western samples.39,40 There are 2 interpretations of this difference. One possibility is that onset and progression of schizophrenia causes musical disability (acquired amusia). The other is that some patients with schizophrenia may have had congenital amusia or “tone deafness,” perhaps related to a brain mechanism that also predisposes to schizophrenia (although this remains speculative). Since we did not determine history of tone deafness when interviewing participants, we were not able to evaluate whether the musical deficits were due to acquired or congenital amusia. Family, premorbid and first-episode studies would be useful in clarifying when the musical deficits can be first observed and to what extent the deficits increase during the course of the illness.
Acoustic studies of patients with schizophrenia have demonstrated impaired processing of sound intensity changes,29 and difficulties in extracting emotional meaning from prosody.41,42 Verbal prosodic pitch discrimination has also been reported to be impaired and to correlate with positive symptoms.43 Neuropsychological studies of patients with specific lesions suggest musical processing requires different and higher levels of cognitive function than sound processing.44 Emotions experienced when listening to music are closely related to reward mechanisms through a network of mesolimbic structures, such as the nucleus accumbens and ventral tegmental area.45 These mechanisms involve the neurotransmitter dopamine, which is central to the pathophysiology and treatment of schizophrenia.46,47 Attention can also be drawn to the hippocampus and anterior cingulate cortex. These regions participate in the emotional response to music in health and show altered synaptic mechanisms related to brain plasticity in patients with schizophrenia.48–50
Positive symptoms, negative symptoms and cognitive impairment are core features of schizophrenia.19 In our study, negative symptoms were correlated with the MBEA global score. Patients with schizophrenia also showed a correlation between overall cognitive functions and global musical score. Our mediation study showed an approximately 43% indirect and 57% direct association between negative symptoms and musical deficit via cognitive impairment, indicating that the effects of negative symptoms on musical disability in patients with schizophrenia are only partially explained by cognitive impairment. This is consistent with reports indicating that negative symptoms and cognitive impairment are strongly correlated, but that they also show discriminative features.22,51–53 Meta-analysis showed that participation in music therapy (7–78 sessions at a frequency of 1–6 sessions per wk for 1–4 mo) resulted in an improvement in negative symptoms, general mental state and some aspects of cognitive function in patients with schizophrenia.54 The association between improvement in symptoms, cognition and possibly in musical ability is not clear.55 Of interest, poststroke studies of indivdiuals with acquired amusia have shown that improvement of verbal memory, attention and executive function was correlated with musical recovery.15,16 Neural plasticity may be the key to rehabilitation of patients with schizophrenia and poststroke and could play a role in recovery of traditionally described cognitive functions as well as musical ability.56 In addition to antipsychotic pharmacotherapy, innovative treatment approaches ranging from music therapy to cognitive remediation to aerobic exercise may represent the application of neuroscience to rehabilitation of neural plasticity in patients with schizophrenia.57–59
Limitations
Since the MBEA was initially established for populations with a Western musical background, cultural differences in music might affect its reliability.10,11 The MBEA global score for controls in this study was comparable with results obtained in Canadian, Chinese and Greek populations.1,4,10 A larger sample size would have allowed us to perform a more detailed comparison of the MBEA subscale results in our homogeneous Japanese sample to results in other racial and cultural groups reported in the literature. The MBEA global score appears to be an effective screening tool for amusia in the Japanese population, but may miss more subtle or domain-specific forms of amusia. Given the age of our participants, it is highly likely that they were all exposed to Western music, even when growing up. More detailed understanding of cultural influences on learning music could have implications for understanding musical abilities in people with mental illness.
The patient and control groups differed in mean level of general education by 2.7 years. Although the shorter duration of education in the patient group was likely associated with the onset of illness, and the extent of musical training did not differ between the groups, lower level of education could contribute to lower MBEA scores in the schizophrenia group. As noted previously, family, premorbid and first-episode studies would help clarify the possible effects of education (both general and musical) on the deficits in musical ability that we observed. Although we observed differences in MBEA global score related to sex as well as correlations with age, the relatively small sample size precluded detailed estimation of these effects over a broad age range or possible interactions. We cannot exclude the possibility that musical training could influence the results, even though these potential confounds did not differ between the groups. A larger sample size would also allow consideration of associations between subscale findings from the MBEA and clinical features of schizophrenia. Identifying dissociations between specific aspects of cognitive impairment and specific musical abilities would provide an opportunity to strengthen the mediation analysis findings with a complementary strategy. Finally, although no correlation was observed between musical ability and antipsychotic medication dose in our study, a larger study with a wider range of medication types and doses is needed to thoroughly examine the possible effects of medication on MBEA scores.
Conclusion
Mean scores in a test of global musical ability were lower than expected in a group of patients with schizophrenia, and most patients were classified as demonstrating amusia. Impaired musical ability was linked to clinical features of illness. Examination of a potential pathway to the deficit identified direct effects of negative symptoms and indirect effects mediated through cognitive impairment. Musical ability may be a unique human attribute and schizophrenia a unique human ailment. Greater understanding of the connection between amusia and schizophrenia could improve our understanding of the neural substrates of functional impairment in people with this illness.
Acknowledgements
We are grateful for the cooperation of all study participants and the assistance of Dr. Yasuhiko Sudo, Dr. Yoichiro Takasaka, and all the staff of Tosa Hospital, Hosogi Unity Hospital and Aki General Hospital. This work was supported by the Kochi Medical School Alumni Association.
Footnotes
Competing interests: A.E. Thornton has a grant from the Mind Foundation of the British Columbia Schizophrenia Society and has received consulting fees from the Provincial Health Services Authority. W.G. Honer has a grant from the Canadian Institutes of Health Research and has received consulting fees from MDH Consulting, Novartis, Roche, Lundbeck, Rush University, the Korean Society for Schizophrenia Research, the Centre for Addiction and Mental Health, the British Columbia Schizophrenia Society, the Fraser Health Authority, the Vancouver Coastal Health Authority, the Provincial Health Services Authority and the Canadian Agency for Drugs and Technology in Health. He is also on the board of In Silico Biosciences. No other competing interests declared.
Contributors: K. Sawada designed the study. S. Hatada, K. Sawada, M. Akamatsu, E. Doi, M. Minese and M. Ramashita acquired the data, which K. Sawada, A.E. Thornton, W.G. Honer and S. Inoue analyzed. S. Hatada, K. Sawada, W.G. Honer and S. Inoue wrote the article, which all authors reviewed and approved for publications.
- Received October 22, 2012.
- Revision received April 15, 2013.
- Revision received June 12, 2013.
- Revision received June 18, 2013.
- Accepted June 25, 2013.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools





